The most important source of light and subsequent energy on earth is the sun. The sun emits energy that can be absorbed by organisms and molecules where it facilitates countless reactions, including photosynthesis, ozone production, vitamin D, and weather phenomena.
Ultraviolet radiation (UVR)
Sunburn and skin cancer are known to be correlated to the dose of UV radiation our skin encounters. UV radiation is emitted by the sun, and is a region in the electromagnetic spectrum between 400-200nm, that can be broken down into three categories: UVA which is between 400-320nm, UVB which is between 320-280nm, and UVC between 280-200nm. As the various types of UV radiation are at different wavelengths, they react differently with the atmosphere. Almost all of the UVC radiation, some of UVB and UVA is absorbed before it reaches the Earth’s surface. The dose of UVA, UVB and UVC changes as UV passes through the atmosphere mainly due to differences in rates of reflection, refraction, scattering and absorption. The change can be emulated on a UV index (Figure 1). A local UV index can be found in a variety of places reporting on meteorological data and forecasts. UVI depicts how much UV radiation is likely to be reaching the Earth’s surface and therefore which precautions should be taken to minimise human risk.

Figure 1. UV index
A UV index value of zero corresponds to no UVR reaching the Earth’s surface, which occurs at night time, and an index of 10 refers to roughly midday sun, when there is no cloud cover. UVR indices record well into the teens when the ozone layer reads low values. The index numbers are measured in watts/meters2, and the measurements reflect different wavelengths to be more harmful than others.
Note that the above precautions are provided for adults with moderately fair to dark skin tone, and that skin damage caused by sun exposure is accumulative over one’s lifetime.
Ozone

Figure 2. Production of ozone in the atmosphere.
As light enters the Earth’s atmosphere, it comes into contact with molecules in the stratosphere. The stratosphere is situated about 10km above sea level and continues up until 50km above sea level. It contains the ozone layer, which absorbs UV radiation. The ozone layer is composed of ozone, a molecule containing 3 oxygen atoms. Oxygen molecules are good absorbers of UVC radiation, using this energy the oxygen bonds break, forming two separate oxygen atoms. These atoms can rejoin, recreating the oxygen molecule, or binding to an oxygen molecule ultimately to form an ozone molecule. Ozone molecules are good absorbers of UVB, and to a lesser degree, UVA. Ozone molecules absorb the energy provided by UVB and UVA to undergo dissociation, releasing oxygen atoms that can combine to form oxygen molecules. These two reactions are in equilibrium, where neither really dominates. Ozone is an important molecule in reducing the amount of harmful UV radiation that passes through our atmosphere, but at low altitudes, such as on the surface of the Earth, it becomes a somewhat toxic and unstable molecule.
The amount of UV light that reaches the Earth’s surface varies and is dependent on a number of factors:
- Latitude: Near the equator, where the sun is directly overhead, the distance from the sun to the ground is the shortest, and the UV has to pass through the least amount of radiation. Therefore, on the equator, the UV intensity is the highest. Likewise, on the poles, the sun appears low in the sky, meaning the light has to pass though more radiation-absorbing atmosphere to reach the surface.
- Elevation: At higher altitudes there is less atmosphere to absorb UV radiation, therefore individuals are exposed to a greater amount of UVR.
- Proximity to an industrial area: photochemical smog produced in industrial processes contains artificially produced ozone. The ozone produced can absorb more UV radiation, but also poses significant health risks if it is low lying.
- Weather conditions: cloud cover can reduce the UV levels on the surface, but often incompletely.
- Reflection: some surfaces are able to reflect UV radiation, meaning there is a greater chance of getting sun burnt, even in shady places. Snow, sand, grass and water are good reflecting surfaces.
- Time of day/year: during the middle of the day, the sun is at its highest position in the sky, resulting in the least distance for radiation to travel, and more exposure to UV light. The summer months also provide the most intense UV radiation, as the sun’s angle (zenith angle) is reduced.
- Ozone layer: the depth of the ozone layer plays a vital role in reducing exposure to UV light. The ozone layer has been found to be thinning in the past few decades. This is presumably due to the release of ozone degrading chemicals by industry.
Ozone depletion
In the past few decades, it has been observed that the ozone layer is thinning over certain regions of the globe, particularly over Antarctica. This has been attributed to chemicals that have been released by industry since the 1930’s, particularly gaseous chlorine and bromine containing substances, such as chlorofluorocarbons (CFC’s) and bromofluorocarbons (BFC’s).
Ozone can be broken down by natural and manmade sources. Atomic chlorine and bromine are two significant contributors, and can be released into the atmosphere by large volcanic eruptions and are also present in chemicals, especially those that where used by industry decades ago, such as CFC’s and BFC’s. CFC’s have been produced as a substitute for toxic and flammable chemicals used in industry, such as ammonia. They’re non-toxic, non-flammable, and their very stable nature made them perfect for propellants in aerosol cans and refrigerants. Their use have grown exponentially (in 1988 it was estimated that over one billion kilograms were being produced annually worldwide) until the discovery that CFS had the capacity of thinning the ozone layer. At this stage world leaders acted by signing the Montreal Protocol, which stipulated that consuming and producing chemicals capable of breaking down ozone be phased out by 2000.
CFC and other similar chemicals are so stable that they’re not destroyed in the troposphere, as they slowly rise towards the stratosphere. These stratospheric molecules are found to be able to break ozone down into an oxygen atom and molecule. This usually occurs at a slow rate, reducing the overall thickness of the ozone layer by about 4% per decade, but in the atmosphere above Antarctica, especially in spring, thinning occurs at an alarming rate. During its winter, Antarctica becomes cold enough (-80°C) for stratospheric clouds (termed Stratospheric Clouds Mother of Pearl, PSCs) to form in the ozone layer. On the surface of these clouds, chlorine and bromine are transformed into an active state and when the sun gains intensity in the spring, clouds disappear freeing chlorine and bromine to rapidly destroy ozone. As temperatures further continue to warm, wind vortexes holding the particles above Antarctica break up, mostly allowing ozone rich air to flow into ‘the hole’. The chlorine and other molecules capable of breaking ozone down can destroy up to a thousand molecules of ozone before it is converted into an inactive form, such as hydrochloric acid.
There are many complex reactions that destroy ozone, the simplest being: a free chlorine atom reacts with an ozone molecule, forming a chlorine and oxygen complex, ClO and an oxygen molecule, O2. The ClO then reacts with a free oxygen atom forming an oxygen molecule and a free chlorine atom. In this manner a circular process is initiated.
Although the Montreal Protocol, first signed in late 1988, will help assist to reduce the effects of destructive radicals in the atmosphere, the effects will not be instantaneous. As it takes years for the CFC’s and other molecules to reach the stratosphere, the reduction in emissions will have minimal effect in the stratosphere (the largest dimension of the hole over Antarctica was measured in 2006, being over three times the size of Australia). It is anticipated that it will take a decade before confirmation of recovery of the ozone can be given.
With the thinning of the ozone layer, less UVB radiation is absorbed resulting in more harmful radiation passing to the Earth’s surface. This would result in increased incidence of skin cancer, cataracts, and other UV related diseases.
Definitions and focus

Figure 3. A typical wavelength.

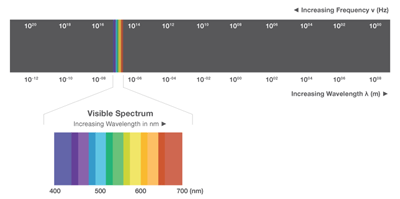
Figure 4. Electromagnetic spectrum.
The energy in the light emitted by the sun and all other sources, travels as mass-less, charge-less particles, photons. Photons can travel as both particles and waves, where each beam of light has its own wavelength (measured peak to peak: Figure 3), frequency (number of wave cycles passing a point per second, Hertz) and energy.
The wavelengths of visible light range from 400nm to 700nm. Once the wavelength drops outside of these values a different form of electromagnetic radiation transpires; these different forms can be found on an electromagnetic spectrum (Figure 4). As evident on Figure 4, the two main sources of electromagnetic radiation emitted by the sun (visible light and ultraviolet radiation – UVR) only occupy a small section of the spectrum.
Environment
The heat supplied by the sun has provided us with a suitable environment to survive. Once radiating energy is passed through the atmosphere, the photons collide with matter, transferring energy. This causes heat, wind, rain, clouds and other weather phenomena. Wind is a result of the varying temperatures of the air above land and water. The hot air rises, causing a flow of cooler air to occupy its previous place, and eventually cool air, high in the atmosphere, drops down to sea level, completing the cycle. When ocean water is heated, water particles evaporate into the air, where they culminate to form clouds. These clouds pushed over land by winds experience lower temperatures, causing condensation into droplets and precipitation. Differences in atmospheric moisture, pressure and temperature result in dramatic weather conditions as hurricanes, cyclones and tornadoes.
When the sun’s rays are shone on an organism, it can have harmful consequences. Different types of electromagnetic radiation have various effects on tissue and DNA. The ultraviolet region of the electromagnetic spectrum can cause serious damage to organic tissues, including human tissue. Humans are protected against ultraviolet radiation by various natural defense mechanisms. Ultraviolet radiation (UVR) can also cause damage to our eyes, both short and long term.
For instance the conjunctiva of the eye may show inflammatory reactions when exposed to intense UVR. Long-term eye (ophtalmis) exposure to sun may have deleterious effects on the retina, causing immediate, and sometimes permanent, visual loss. Long-term UV exposure contributes to cataract formation.
Photosynthesis

Figure 5. The process of photosynthesis.
Photosynthesis is a process carried out by photo-autotrophs.Put simply, photosynthesis is water and carbon dioxide, in the presence of light, forming oxygen and glucose.
The oxygen produced is released out into the atmosphere through stomata while the carbohydrate, glucose, can be modified to produce various other carbohydrates, such as cellulose for plant walls, or starch, a glucose storage molecule.
The carbon dioxide is acquired through stomata, small gaps in plant leaves that are surrounded by two guard cells. These guard cells are able to open and close depending on the environmental conditions. For instance, if conditions are extremely dry, guard cells would swell to close the gaps, in order to minimize water loss. These gaps allow carbon dioxide and water vapor to enter the plant, and oxygen and water vapor to leave. In turn, water is acquired through the plant roots. Moisture obtained from the soil may travel through the roots up the plant to the leaves via the xylem (vascular tissue). The xylem is a tissue in vascular plants that carries water and minerals from the roots, to all other sections of a plant.

Figure 6. Diagram of a chloroplast.
The energy within the sunlight is captured by chlorophyll, a pigment found in chloroplasts. Chlorophyll is of biological relevance due to its chemical structure, and subsequent absorption spectra. Also present in chloroplasts and involved in photosynthesis are grana, which are stacks of thylakoid discs, and the stroma, which is a dense fluid surrounding the grana (see Figure 6).
Photosynthesis is separated into two phases: the light dependent and independent stages. The light dependent stage involves the absorption of a photon and its conversion to an electron, a series of reactions follows, which conclude in an oxygen molecule being released into the atmosphere. The light independent reaction involves the absorption of carbon dioxide by an enzyme, RuBisCO, and results in the production of carbohydrates.
Light dependent reaction

Figure 7. Diagram of a photosystem.
The light dependent reaction can occur by two mechanisms: cyclic photophosphorylation and non-cyclic photophosphorylation. Non-cyclic photophosphorylation is the more common of the two in plants, produces ATP and NADPH and involves the use of two photosystems, photosystem I and II. Cyclic photophosphorylation occurs in plants when there is insufficient NADP+ to produce NADPH, involves photosystem I and only produces ATP.
A photosystem is an arrangement of pigments, such as chlorophyll, packed into a thylakoid membrane. The energy containing packets in light (photons) are absorbed by accessory pigments, passed to the primary pigment, and then collected where they initiate the production of energy in the form of ATP and NADPH. The primary pigment associated with photosystem I is P700, while P680 is associated with photosystem II. These numbers 700 and 680, refer to the wavelengths of light that the respective pigments can absorb.

Figure 8. Non-Cyclic photophosphorylation reaction.
Non-cyclic photophosphorylation (Figure 8) begins with photosystem 2. The photons present in light are absorbed by P680, where they excite an electron. This electron is then passed to a primary electron acceptor molecule through a process termed photoinduced charge separation. The positive charge left on the P680 molecule is alleviated by the extraction of electrons from water molecules, causing the release of atomic oxygen. The electron held by the primary electron acceptor is passed to pheophyton then down the electron transport chain. This creates a chemiosmotic gradient which leads to ATP being formed by ATP synthase in the light independent reaction. Once passed through the electron transport chain, the electron enters photosystem 1 where it is re-excited and begins its path down another electron chain. The electron is again passed through a series of reactions, eventually being added to NADP+ reductase to form NADPH.

Figure 9. Cyclic photophosphorylation reaction.
Cyclic photophosphorylation only involves photosystem 1. P700 absorbs photons until an electron is raised to its excited state. The electron then passed undergoes photoinduced charge separation, before being passed down an electron transport chain, producing a chemiosmotic potential across the membrane. This ion gradient stimulates the production of ATP from ATP synthase. Once the electron reaches the end of the electron chain, it is passed back to the photosystem by electron acceptor molecules (see Figure 9). Cyclic photophosphorylation also occurs in certain photosynthetic bacteria.
Light independent reaction

Figure 10. Light independent reaction.
Light independent reactions are also referred to as carbon fixation. Ribulose biophosphate (RuBP), with assistance from the enzyme RuBisCo, is combined with a carbon dioxide molecule. The end product is two, three-carbon, 3-phosphoglycerate (PGA), molecules. The ATP and NADPH produced in the light dependent reaction are used to reduce PGA to 3-phosphoglyceraldehyde (PGAL). Additionally, 5 of every 6 molecules of PGAL produced are reused in the production of RuBP, while the remaining molecule is used in the formation of carbohydrates, such as starch, cellulose and glucose (Figure 10).
References
- Cartage.org, (2007). Photosynthesis [Online]. Available from: http://www.cartage.org.lb/en/themes/sciences/BotanicalSciences/Photosynthesis/Photosynthesis/Photosynthesis.htm [Accessed on 29/04/2008].
- de Gruijl, F R, Longstreth, J, Norval, M, Cullen, A P, Slaper, H, Kripke, M L, Takizawa, Y, (2003). Health effects from stratospheric ozone depletion and interactions with climate change, Photochemistry and Photobiology. Vol 2, pp 16-28.
- Helpsavetheclimate.com, (2007). Photosynthesis [Online]. Available from: http://www.helpsavetheclimate.com/photosynthesis.html [Accessed on 29/04/2008].
- Slaper, H, Velders, G J, Daniel, J S, de Gruijl, F R, van der Leun, J C, (1996) Estimates of ozone depletion and skin cancer incidence to examine the Vienna Convention achievements, Nature. Vol 384(6606). pp 256-258.
- Solcomhouse.com, (2006). Ozone [Online]. Available from: http://www.solcomhouse.com/ozone.htm [Accessed on 29/04/2008].